

About Lehe
乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。




Overview of the illness
In October 2021, Mr. Zhao presented to the hospital primarily due to "choking while eating and discomfort in the right chest". On October 22, a chest and upper abdominal CT scan revealed localized wall thickening of the esophagus, consistent with CT findings of a tumor. Multiple small lymph nodes were also observed in the mediastinum.
On November 1st, gastroscopy revealed esophageal lesions pending pathology (CA to be excluded). Endoscopic ultrasonography showed early Ca (T1) in the mid-esophagus. On November 2nd, esophageal mucosal ESD was performed. Postoperative pathology indicated: (esophageal ESD specimen) high-grade intraepithelial neoplasia with focal malignant transformation into moderately differentiated squamous cell carcinoma, accompanied by involvement of esophageal glandular ducts. Gross classification was Type 0-IIb. The (microscopically) lesion range was 3.3x3cm, of which the squamous cell carcinoma lesion range was 3.3x1.3cm. (Smooth muscle of the mucosa was present.) Histological typing of the deepest infiltrating cancer tissue was moderately differentiated squamous cell carcinoma. Infiltration pattern: INFb. No definite intravascular tumor thrombus was detected (ly0v0). No lesions were detected along the horizontal tangent line of the specimen (pHMO), but adjacent to the vertical tangent line (pVM1). Immunohistochemistry: CD34 (vascular +), D2-40 (lymphatic +).
On November 26th, the PET-CT scan revealed the following: 1. Postoperative changes in the esophagus due to cancer surgery; 2. Multiple small lymph nodes in the mediastinum without abnormal high metabolism, observation recommended; 3. Micro-nodules in both lungs without abnormal high metabolism, observation recommended; left lung with fibrous streaks.
On December 23, a robot-assisted partial resection of the esophagus and stomach, cervical esophagogastric anastomosis, lymph node dissection, and bilateral recurrent laryngeal nerve dissection were performed. Postoperative pathology: "post-ESD surgery for esophageal malignancy in another hospital" revealed focal loss of esophageal mucosa, accompanied by hemorrhage, fibrosis, and minimal lymphocyte infiltration and multinucleated giant cell reaction in the submucosa, consistent with post-ESD reaction. No tumor was found at the superior, inferior, or circumferential resection margins. Glycogenosis acanthosis was observed in the surrounding esophageal mucosa. No significant lesions were found in the surrounding gastric mucosa. Metastatic squamous cell carcinoma was found in the lymph nodes (4/37), without involvement of the lymph node capsule. pTNM: pT1N2 (T staging combined with post-ESD pathology) stage IIB.
Lehe New Medical [Second Diagnosis and Treatment Suggestion]
1. Mr. Zhao's pathological stage is ⅡB, with lymph node metastasis present. In this case, the recurrence probability of simple surgical resection is extremely high. Therefore, adjuvant therapy should be actively pursued after surgery to further eliminate residual tumor cells and achieve the goal of controlling tumor recurrence.
2. Multiple studies suggest that postoperative adjuvant radiotherapy can improve the prognosis of patients with positive lymph nodes after undergoing surgery alone, and the efficacy of radiotherapy combined with chemotherapy is superior to that of radiotherapy alone. Currently, adjuvant therapy for esophageal cancer surgery primarily involves chemotherapy. However, for patients with esophageal cancer, chemotherapy has a low response rate and poor therapeutic effect, with an objective response rate of only 6%-8%. It can only exert a killing and inhibitory effect on tumor cells in the short term and is associated with drug resistance; in addition, chemotherapy has significant side effects, severely damaging the immune system and hematopoietic system, and cannot achieve long-term efficacy. Therefore, it is not an ideal adjuvant therapy after surgery.
3. vNKT cell immunotherapy is a novel anti-tumor treatment method that utilizes the potent killing effect of immune cells on tumors. It can eliminate residual or newly emerging tumor cells, reconstruct the immune microenvironment, and restore the body's immune system's ability to clear tumors, without the toxic side effects and drug resistance issues associated with traditional chemotherapy. Extensive clinical practice has confirmed that combining vNKT cell therapy with surgical treatment can effectively reduce the risk of recurrent and newly emerging tumors, making it an ideal choice for postoperative adjuvant therapy and highly suitable as a subsequent treatment option for Mr. Zhao.
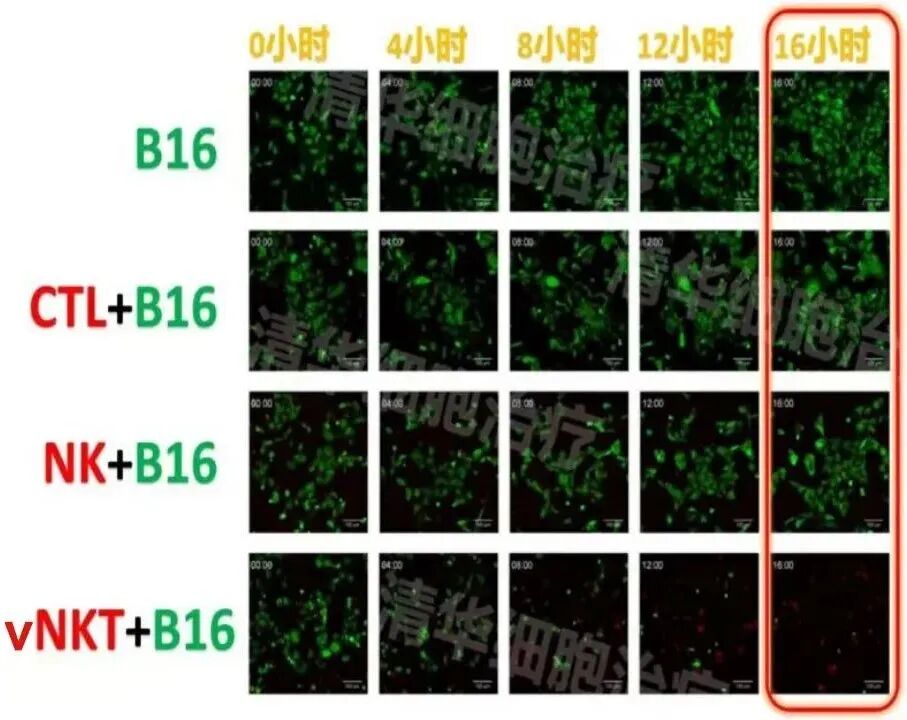
Experimental conditions: In the presence of vNKT cells, after 16 hours, nearly all B16 tumor cells were killed!
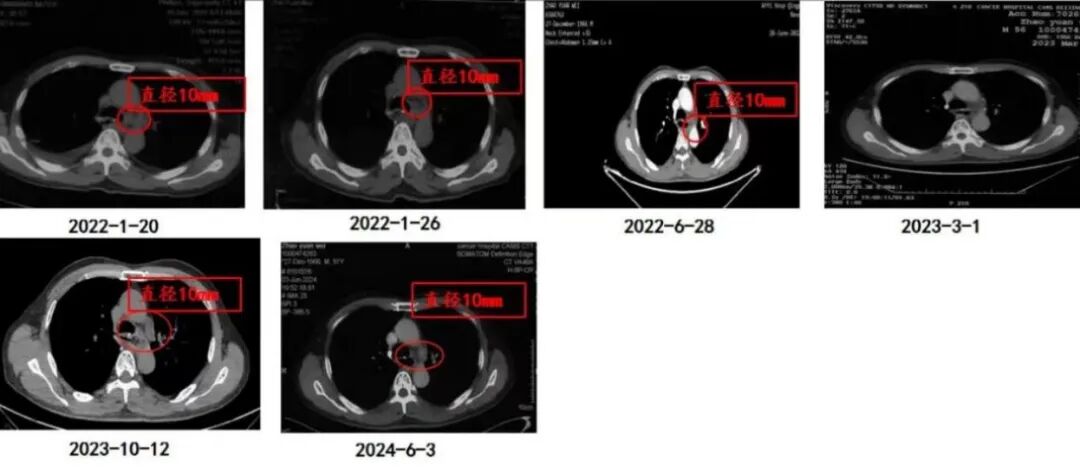
Imaging changes
Conclusion and Commentary



Scan QR code
Communicate with Professor Zhang Minghui's team
Click on the image to view the exciting content from previous issues



Address: Room 1101 (Unit 101), 11th Floor, Building 1, No. 7 Courtyard, Kexueyuan Road, Life Science Park, Changping District, Beijing
Phone:010-8265 9866
Email:lehemedneo@hotmail.com